If you’d like to discuss One Anastomosis Gastric Bypass, Roux-en-Y or other surgical and non-surgical weight loss options, contact us anytime to schedule an appointment with a member of the team.
WHAT IS A ONE ANASTOMOSIS GASTRIC BYPASS?
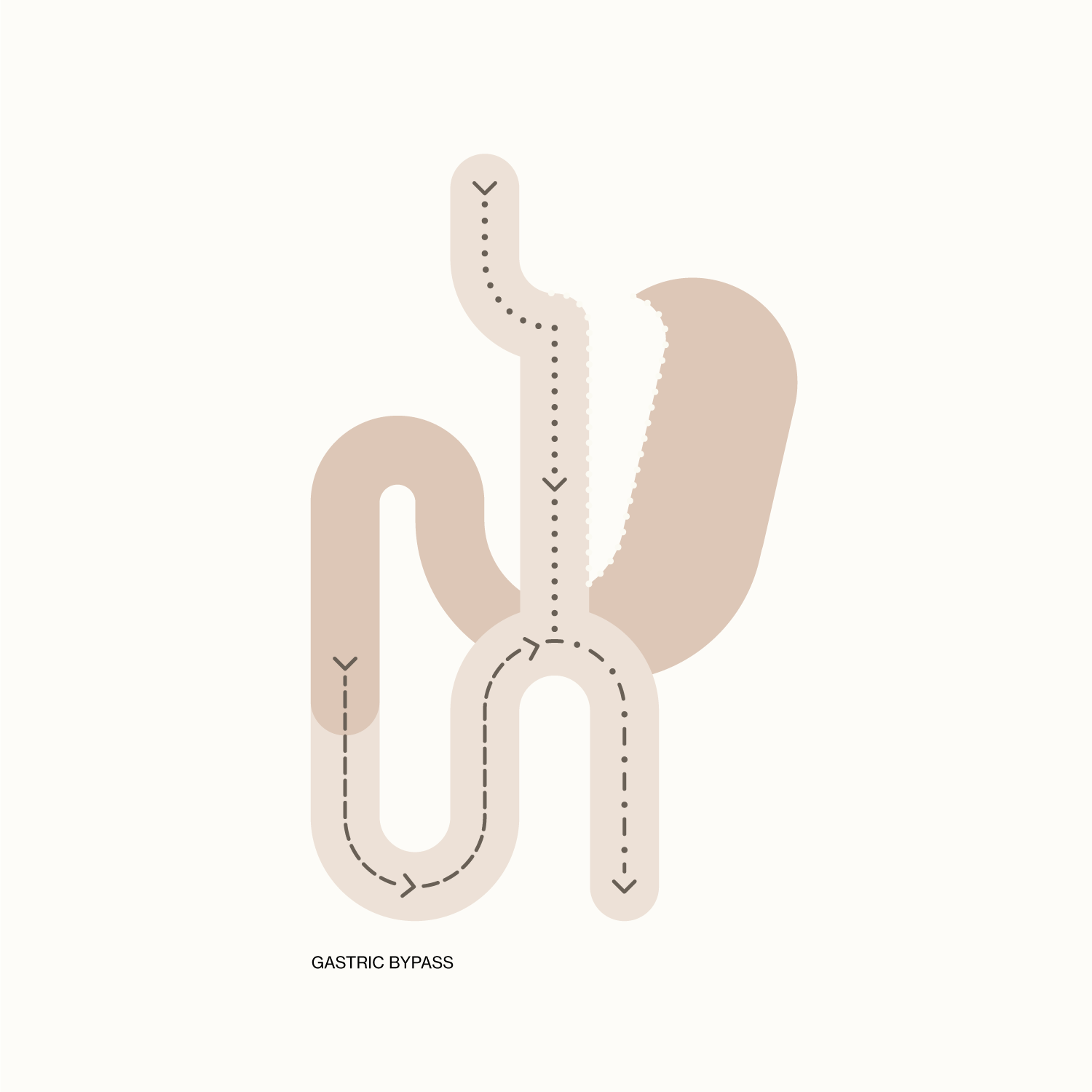
One anastomosis gastric bypass (OAGB) is a type of gastric bypass and is also known as a single anastomosis gastric bypass, mini-bypass or even omega-loop bypass.
‘One anastomosis gastric bypass’ refers to there only being one join between the stomach and the small bowel. This is compared to a Roux-en-Y gastric bypass, which has an added join between two parts of small bowel.
The one anastomosis bypass is performed laparoscopically, or keyhole, through 5 small cuts to your abdomen. The ‘mini-bypass’ is an operation that Dr Balalis performs as a primary surgery, a surgery for someone who has not had other weight loss surgeries previously, or a revision operation.
This surgical procedure involves using a bougie, or plastic tube, inserted through the mouth to guide the creation of a small stomach pouch. The stomach pouch is then joined to the bowel, 150cms from the start of the duodenal-jejunal (DJ) flexure (a part of the small bowel).
WHO IS ELIGIBLE FOR A ONE ANASTOMOSIS GASTRIC BYPASS?
Guidelines include:
- Age >18
- BMI 30 with weight related comorbidities
- Or BMI ≥ 35 with no comorbidities needed
- No eating disorders
- No untreated acute psychiatric disorders
- No alcohol or drug dependency
- Has tried other avenues without success
- Committed to a healthy lifestyle and lifelong care
Note: these are guidelines, and all patients require a discussion regarding one anastomosis gastric bypass and other forms of bariatric surgery.
HOW DOES THE ONE ANASTOMOSIS GASTRIC BYPASS WORK?
The one anastomosis gastric bypass works by both decreasing the volume of the gastric pouch as well as providing hormonal changes by bypassing the duodenum and part of the jejunum. This results in a decrease in levels of hunger, as well as a feeling of fullness with a smaller amount of food. There are also changes to absorption by bypassing over 150cms of your small bowel.
HOW MUCH WEIGHT CAN I EXPECT TO LOSE?
Patients can expect to lose around 65-75% of excess weight, with the majority occurring in the first year.
WHAT DOES THIS MEAN?
For an example, a 176cm patient who weighs 140kgs, has a BMI of 45. Their ideal weight is 78kgs (for a BMI 25), which means an excess weight of 62kgs. This means that 70% of this is 43kgs, and this patient can expect to end up at around 97kgs as a rough guide.
WHAT ARE SOME OF THE POTENTIAL HEALTH BENEFITS?
One-anastomosis gastric bypass is also effective at normalising diabetes, blood pressure, high cholesterol and sleep apnoea to name a few. Trials have shown that in patients with type 2 diabetes, at 3 years over 60% have normal blood sugars.
WHAT ARE THE RISKS?
A serious risk is a leak, which is very rare (<1% Australia wide) but may need a further operation to manage. It is always important to detect these issues early, and this is part of the reason why Dr Balalis performs post-operative assessments for all his patients. He undertakes a CT abdomen with oral contrast before you leave hospital to ensure normal passage of contrast prior to upgrading your diet. Dr Balalis also sees his patients regularly (at least once a day) before they are discharged.
Another risk is an ulcer at the join between the stomach and bowel (anastomosis). This ulcer is more likely to occur in patients who take up smoking again or use anti-inflammatories.
Anti-inflammatories, such as Nurofen, Mobic, Voltaren, or Prednisolone increase the risk of ulceration significantly and cannot be taken at all with a bypass. An ulcer can cause pain, can bleed and even perforate. Smoking is another risk factor for ulcers and cannot be undertaken at all following a gastric bypass. This is also true for at least 6 weeks prior to any operation. Dr Balalis will discuss this further with patients during consultation.
Another issue with the one anastomosis gastric bypass is bile reflux. This may result in an unpleasant taste in the patient’s mouth, and acid reducing medication does not improve these symptoms. A Roux-en-Y bypass may be required in around 1-2% of patients to resolve bile reflux.
Patients require regular nutritional monitoring following their one anastomosis gastric bypass and need to continue a multivitamin long-term.
As with all weight loss surgeries performed, it is important to continue to work with your multidisciplinary team towards long-lasting good habits and routines.